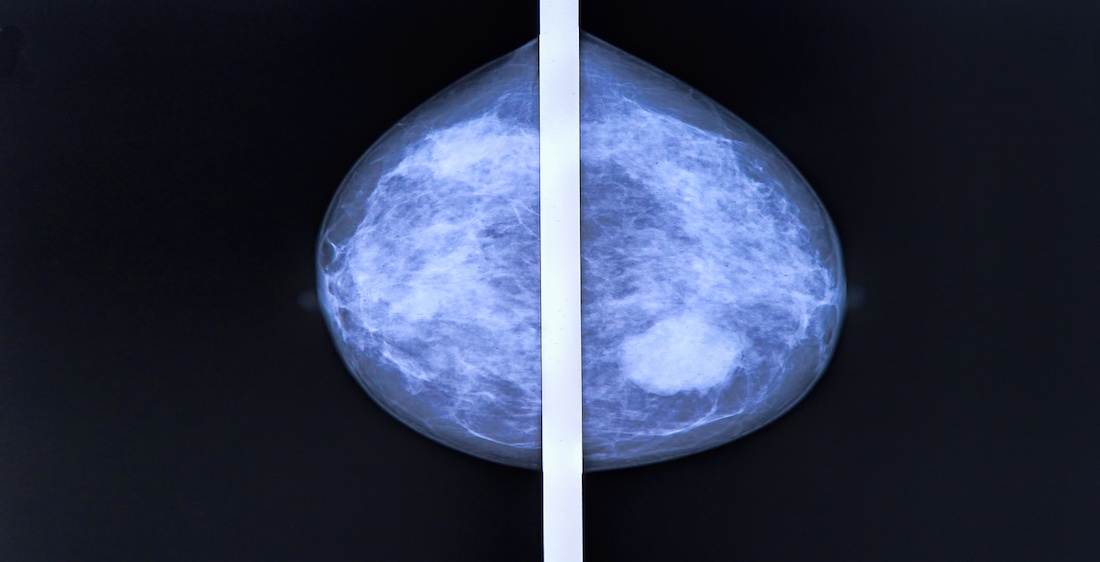
Upon diagnosis of breast cancer, a woman is faced with two grave choices: either have a less-radical lumpectomy or the dreaded mastectomy.
A lumpectomy is done on a person who is in the clinical stage I or II of breast cancer. Also known as the breast conservation surgery, it is performed by removing the tumor or the lump in a breast.
On the other hand, mastectomy is a more challenging choice. It is performed by removing the whole breast to prevent the spread of the cancer. It can either be done as a single mastectomy, where only one breast is surgically removed, or a double mastectomy where both are removed.
In 2013, actress Angelina Jolie received praise for her courage for voluntarily undergoing a double mastectomy to prevent her from contracting breast cancer, a condition she had an 87 percent chance of getting due to her genetic history.
Whatever the case, women who have undergone these preventive surgeries are left with chests that may make them feel less of a woman than before. It is reported that women’s state post-mastectomy can range from traumatized to depressed. (Find the breast cancer facts you need: Breast cancer awareness)
However, with constant developments in plastic surgery, it is now possible to help these courageous women feel even better about themselves particularly through breast reconstruction surgery.
The procedure has been traced back to as far as the 1800’s. Now, it is one of the leading plastic surgery operations in the US with a 2012 statistic from the American Society of Plastic Surgeons (APSP) showing 91,655 operations performed in that year.
The types of operations used in breast reconstruction are as follows:
Implant Procedures
Breast implant procedures are operations wherein implant shells are placed under the skin where the breast used to be. Implant procedures are usually done with:
Silicone implants made of silicone elastomer filled with silicone gels. They are generally considered to be softer and feel more like breast tissue. Saline implants are filled with a salt water solution. Some patients remark that saline implants feel stiffer and unnatural but require a smaller incision during surgery. It also poses very low health risks.
Breast reconstruction can be one-stage immediate or direct-to-implant, where a permanent implant is inserted immediately following a mastectomy. After the breast surgeon removes the breast tissue, a plastic surgeon places an implant in its place.
When tissue in the breasts is not healthy enough to support a full-sized implant right away, a two-stage reconstruction is a better option. A short-term tissue expander is placed in the breast tissue for two to three months to allow the skin flaps in the breast to stretch. When the breast tissue is ready, a tiny valve is inserted under the skin by a surgeon to inject a salt-water solution at regular intervals to gradually fill the expander. When the skin is stretched enough, a second surgery will remove the expander and put in the permanent implant. In some cases, surgeons leave the expanders in place as the final implant.
Tissue Flap Procedures
Tissue flap surgery takes tissue from the stomach, back, thighs, or buttocks and substitute as substitute for breast tissue and rebuild the breast shape. There are several ways to perform the procedure:
Abdominal flap surgery can either be TRAM (transverse rectus abdominis muscle) or DIEP. The former culls tissue and muscle from the stomach, while the latter takes only tissue from the same area.
Latissimus dorsi flap reconstruction transfers muscle, fat, skin, and blood vessels from the upper back and under the skin to the front of the chest. This results in more natural-looking breasts.
Gluteal free flap or GAP (gluteal artery perforator) surgery is performed on women who are either too thin or too hesitant to make incisions on the tummy. It uses tissue from the buttocks and the gluteal muscle to achieve a better breast shape.
Inner thigh or the TUG (transverse upper gracilis) flap procedure is a new alternative for women who find other flaps incompatible with their reconstruction needs. The inner thigh flap, composed of skin, fat, muscle, and blood vessels, is re-attached to the chest through microsurgery.




Recent Comments